Authored by: David C. Buck, M.D. - Orthopedic Surgeon and Sports Medicine Specialist at MD West ONE (Omaha and Fremont, Nebraska)
The meniscal root is a complex of ligaments and meniscal attachments to the tibia (shin bone). Meniscal root tears are an avulsion of the meniscal cartilage at the attachment to the tibia. These injuries occur within 1 cm of the attachment and can lead to meniscal instability and extrusion. The meniscal roots have an important function for the meniscus to convert weight bearing and twisting loads into hoop stresses and act as a shock absorber for your knee. These injuries can lead to significant pain, instability, and development of arthritis within the knee. Root tears will cause the meniscus to extrude from the joint, which changes the biomechanics of the knee. This can lead to arthritis, insufficiency fractures, and accelerated degeneration of the knee joint.
These injuries often occur with a twisting or rotational force. They often occur while loading the knee with weights. They can also occur during sports activities or with a traumatic injury onset. We have seen and treated these injuries in children as young as 11 and adults into their early 60s.
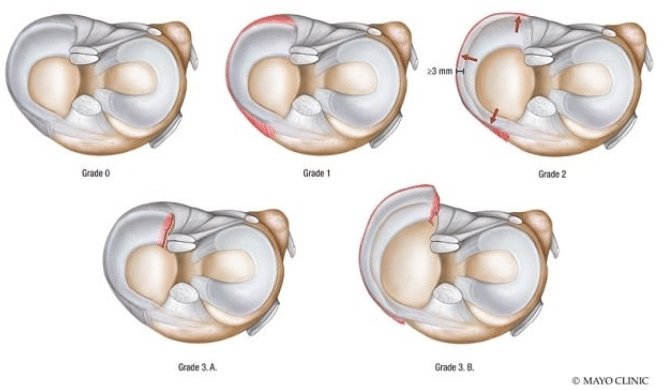
Classification of meniscus extrusion and tear, MTL and MMPR grading system. Classification of meniscus extrusion and tear, meniscotibial ligament (MTL), and medial meniscus posterior root grading system. The?MTL?fails in the extrusion state, leading to concentrated forces at the root which then result in root tear. (Mayo Clinic)

Dr. David Buck
Orthopedic Sports Medicine Specialist
Emerging focus on meniscus root tears
In recent years, we have recognized the significance of these injuries. The decision to proceed surgically with repair, especially in younger patients or those with mild arthritis, is crucial. Without surgery, the healing potential for these meniscal root injuries is poor and can lead to progressive pain, instability, and arthritis. The literature reports a non-operative natural history of 95% failure (Krych et al, American Journal of Sports Medicine, 2023).
Clinical Evaluation
A high degree of suspicion is required in the presence of risk factors. Patients can report joint line pain and mechanical symptoms (locking, catching and giving way) but is not present in all patients. Some patients may hear of feel a popping sound during light activities. The most common findings on physical examination are pain with full knee flexion, joint line tenderness, and a positive McMurray test with the surgeon palpating the extruding meniscus during examination.
Imaging
Magnetic resonance imaging (MRI) is the imaging study of choice. This can help to diagnose meniscal root tears as well as other pathology which can be present including insufficiency fractures and bone marrow edema.
Treatment
Treatment of meniscal root tears is variable based upon the severity of the injury, timing of injury to surgical intervention and the condition of the articular cartilage and degree of arthritis in the joint. The goal of surgery is to restore the natural biomechanics of the knee in order to delay the development of arthritis. Therefore, surgical repair is not indicated for patients with advanced arthritis.
Non-Operative Treatment
Elderly patients with advanced arthritis are candidates for non-operative treatment. Symptomatic treatment with use of analgesics, (oral or topical), corticosteroid injections, activity modifications and a knee brace can relieve some of the symptoms. Treatment is based on the arthritis rather than the meniscal root tear and can include performing a knee replacement.
Meniscal Root Repair Surgery
Performing a knee arthroscopy to include an anatomic repair of the meniscal root should be attempted whenever possible to prevent further meniscus damage and the development and progression of arthritis.
Meniscal root repairs have been reported to improve subjective patient outcomes. Several recent studies in the literature have shown improved clinical scores and a decreased rate of conversion to knee replacement following injury.
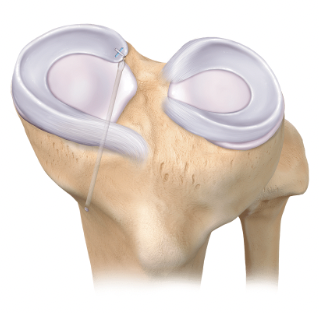
Personally, I use the Arthrex Suture-Loc repair system. It allows for direct fixation of the meniscal root and uses a small cannulated drill pin to facilitate the anatomic repair.
This shows the Suture-Loc device, loaded with two sutures, and passed through a 2.4mm cannulated drill bit, to facilitate repair.

Intra-operative arthroscopy images showing the avulsed meniscal root from the anatomic attachment on the tibia.
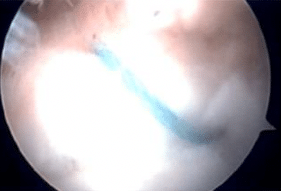
Repair sutures (x2) passed through meniscal root tissue and repaired down to the anatomic footprint on the tibia.
Postoperative Rehabilitation and Recovery Course
Following surgery, I will keep patients non-weight bearing for 4-6 weeks using crutches. I instruct them to keep the incisions clean and dry for 4 weeks. A short course of post-operative pain medications will be prescribed. Physical therapy goals include regaining range of motion of the knee, decreasing swelling, and maintaining muscle tone. Patients can begin weight bearing after the initial protected period. Return to sports and heavy labor work activities is likely at 12 weeks.
Personal Note from Dr. Buck:
A meniscal root tear injury can be a complex injury for patients and can be a longer recovery process compared to other knee scope procedures. Our goal is to help you work-up and evaluate the injury, have a successful surgery if needed, and return to sports and activities at the highest level. We are here to help you navigate this process and our goal is to get you back to all of your activities in a safe and timely manner.
About Dr. Buck:
Dr. Buck is a Board-Certified Orthopedic Surgeon with a Certificate of Added Qualification as a Sports Medicine Specialist with MD West ONE.
Dr. Buck serves as the Team Physician for Midland University and also is a part of the Sports Medicine team providing coverage for the NCAA College World Series in Omaha. He works closely with several local area high schools and their sports medicine programs. Dr. Buck is a former Certified Athletic Trainer as well as an athlete and coach. He can be reached at (402) 721-0090 to schedule an appointment at either our Elkhorn (192nd & Dodge) or Fremont locations.