

Authored by: David C. Buck, M.D. - Orthopedic Surgeon and Sports Medicine Specialist at MD West ONE (Omaha and Fremont, Nebraska)
Ankle sprains are one of the most common injuries we see in athletes. The ankle joint is formed by three bones in the lower leg. These are the tibia (shin bone), fibula (outside), and talus (the dome shaped bone below the tibia). A ligament is a band of connective tissue that connects bone to bone and provides stability to a joint. This combination of ankle bones and ligaments make up the ankle joint.
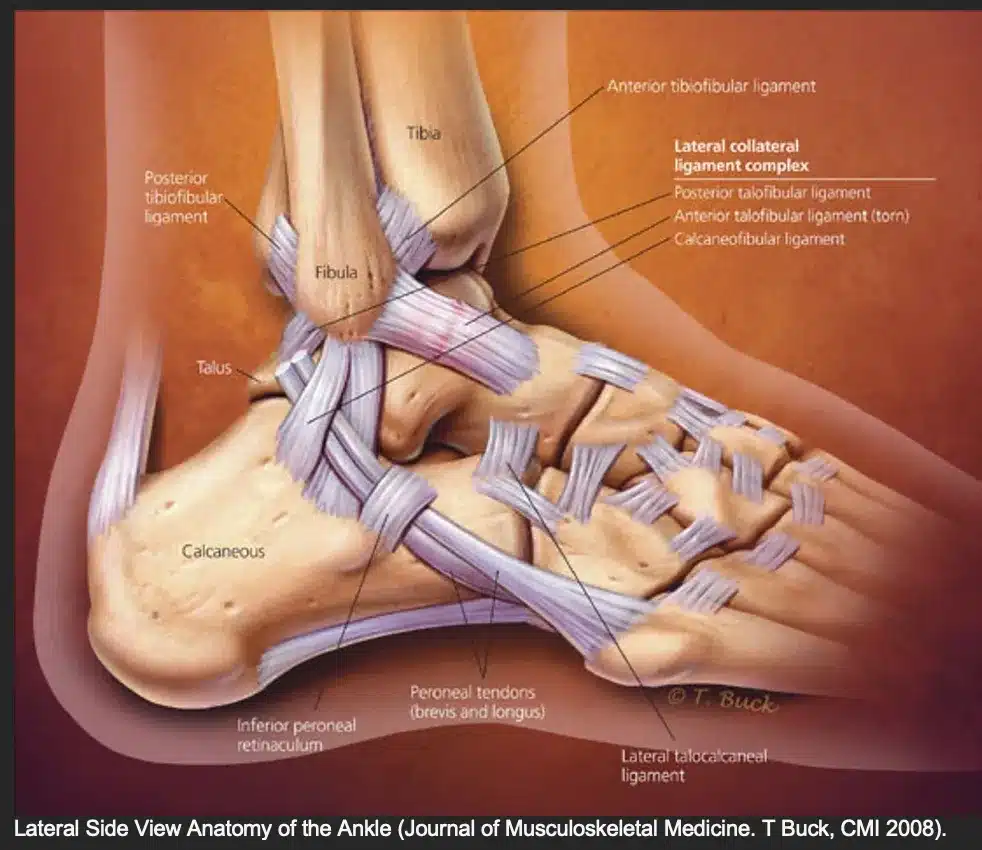

A high ankle sprain involves different ligaments than the more common lateral ankle sprain. The ligaments injured in a high ankle sprain are located above the ankle joint and are located between the tibia and fibula. They form what is known as the syndesmosis and have both an anterior (front) and posterior (back) tibiofibular ligament as well as the interosseous membrane that connects the tibia and fibula up into the lower leg. When you bear weight on the leg during sports, the tibia and fibula experience high forces that want to spread and separate these bones. The ligaments of the syndesmosis serve as a type of shock absorber and stabilizer to keep these bones together during dynamic athletic activities.
A high ankle sprain often occurs in contact or collision sports when the ankle rolls outward with the ankle in a dorsiflexed position (the foot rotates outward while the ankle bends upward towards the shinbone). Following this type of injury, athletes are often unable to bear weight. Moderate swelling and/or bruising is often noted following the injury. Pain is localized over the front of the ankle extending up the leg. There is pain when squeezing the lower leg together as well as pain extending >5cm up from the ankle itself. There is also pain or instability when the ankle is rotated outwards with the ankle in a dorsiflexed position, essentially recreating the injury mechanism.
Immediate management includes RICE (rest, ice, compression, and elevation), immobilization in a CAM boot, and protected weight bearing with crutches. I will often begin prescription anti-inflammatories to help reduce swelling and inflammation. I will obtain x-rays to rule out a fracture and often an MRI to fully evaluate the injury. If there is significant injury to the syndesmosis ligaments, then I will recommend surgery to stabilize the ankle joint using the Arthrex TIGHTROPE implant device.
When surgery is indicated for a high ankle sprain, I will first begin with an arthroscopic evaluation of the ankle. This will allow for any articular cartilage injuries to be managed, assess the ligaments about the ankle, and debride any inflammation or synovitis from the ankle joint. Next, I will make a small incision (2-3cm) over the lateral ankle over the fibula. A small plate is placed and secured to the fibula. The ankle mortise and syndesmosis are then reduced and confirmed with an intraoperative x-ray. Finally, the syndesmosis is secured by drilling across the fibula and tibia and placing two diverging TIGHTROPE devices. These devices are made of opposing stainless steel buttons and the braided suture which traverses the syndesmosis. This allows for flexible fixation and stabilization of the syndesmosis. The TIGHTROPE function to stabilize the ligamentous complex while the patient’s torn ligaments heal. This allows patients to accelerate their rehabilitation with the end goal of returning to their sport in a more timely fashion.
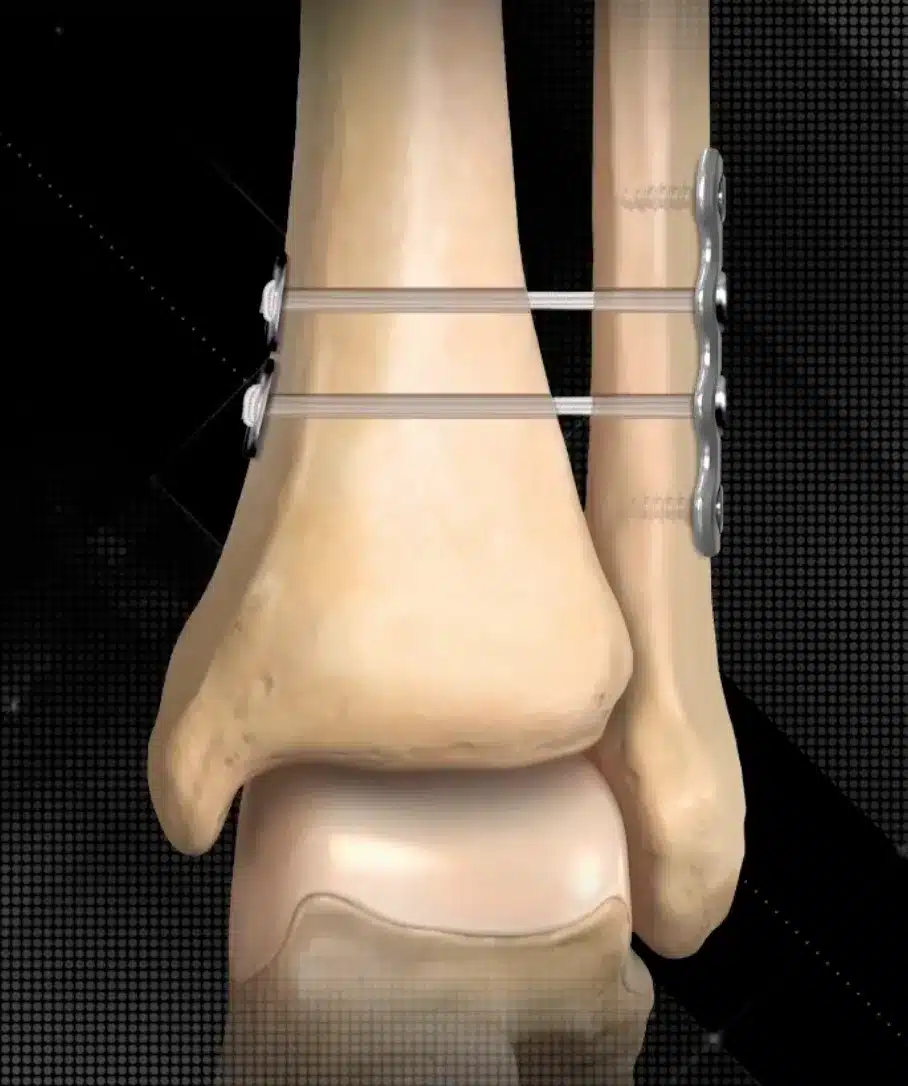
Historically, the gold standard for these unstable injuries has been to place two screws across the syndesmosis to rigidly stabilize the ankle mortise and syndesmosis to allow for healing. These screws would need to be removed in 4 months to prevent breakage and allow for ankle range of motion. The TIGHTROPE device is used to provide a durable and flexible construct that allows early restoration of ankle function, motion, and stability with an accelerated return to sports.
The rehab protocol following TIGHTROPE repair is more accelerated than traditional methods of surgery. I will protect the ankle in the CAM boot early following surgery to allow for swelling control, icing, and elevation. Physical therapy will begin with modalities to help reduce swelling and inflammation on day 1 or 2 following surgery. Athletes will begin walking on day 3-4 in the boot and transition out of the CAM boot by day 7-10. Most athletes can begin light jogging in 10-14 days. I will allow them to advance as pain allows back to sport specific activities including running, cutting, pivoting, and jumping. Typically, athletes may return to sport as pain allows in an ankle brace in 4 weeks following surgery.
The risks of this procedure, which is done in an outpatient same-day surgery, are infection, stiffness, and blood clot. We will provide medications to reduce these risks following surgery. There is also the general risk of anesthesia and the risk of unforeseen medical complications. Overall, this is low-risk procedure with an excellent outcome for stabilizing the ankle and allowing a much earlier return to sport than previous surgical methods. I have performed this procedure personally on many athletes who have returned to basketball, volleyball, football, and soccer sports within 3-6 weeks following repair.
Personal Note from Dr. Buck: A high ankle sprain can be a frustrating and complex injury for young athletes. My goal is to help you evaluate the injury and determine if surgery is the correct way to manage the injury. Over the recent years, the TIGHTROPE procedure for high ankle sprains has become very popular and is becoming the gold standard for surgical treatment. I have worked with athletes over the past several years that have gotten back to their sports at the high school and collegiate level following this procedure. We are here to help you navigate this process and our goal is to get you back to all of your activities in a safe and timely manner.
About Dr. Buck:
Dr. David Buck is a Board-Certified Orthopedic Surgeon with a Certificate of Added Qualification as a Sports Medicine Specialist with MD West ONE. I am proud to again be recently named a Castle Connolly Top Doctor, a national award recognizing physicians that is based both on patient reviews and peer nominations from physician colleagues.
Dr. Buck serves as the Team Physician for Midland University and also is a part of the Sports Medicine team providing coverage for the NCAA College World Series in Omaha. He works closely with several local area high schools and their sports medicine programs. Dr. Buck is a former Certified Athletic Trainer as well as an athlete and coach. He can be reached at (402) 721-0090 to schedule an appointment at either our Elkhorn (192nd & Dodge) or Fremont locations.