
Are you suffering from symptoms of Tennis or Golfer's Elbow?
The Omaha Elbow Specialists at MD West ONE can properly diagnose and treat Tennis/Golfer's Elbow through non-surgical and surgical treatments. If you have the following symptoms, you may want to make an appointment with one of our Board Certified Specialists.
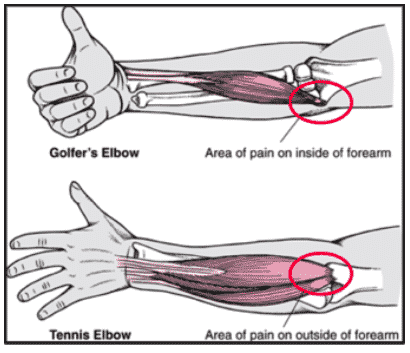
- Tennis Elbow:
- Pain with resisted wrist extension and gripping activities.
- Point tenderness at the Extensor Carpi Radialis Brevis (ECRB) insertion on the outer side of the elbow (epicondyle).
- May experience decreased grip strength.
- Golfer’s Elbow:
- Pain on the inside of the elbow increases with gripping, lifting, and throwing
- Tenderness along the common flexor tendon origin and on the inside of that elbow.
Meet MD West ONE's orthopedic specialists and learn more about how they treat tennis/golfer's elbow...
















Tennis/Golfer's Elbow: Non-surgical and Surgical Treatment(s)
What is Tennis/Golfer's Elbow?
Tendinopathy (breakdown of cartilage in tendon) in the elbow is a very common condition that presents with pain about the inside (medial) or outside (lateral) of the elbow. Pain on the inside of the elbow is commonly referred to golfer’s elbow, and on the outside of the elbow is commonly referred to tennis elbow. Coping with these conditions as they run their course can be quite painful and frustrating.
Tendinopathy in the elbow is the most common cause of elbow pain. It is estimated that between 0.7-3% of the adult population experiences lateral epicondylitis symptoms every year. Most people who are affected by tennis elbow are, in fact not tennis players, but it may effect up to 50% of tennis players in their career. It is most common in people between the 35-55 years old and may be associated with repetitive gripping or lifting tasks. Men and women are equally affected.
This condition is more of an age related change in the tendon origin near the bone. It may be caused by repetitive wrist extension, forearm pronation, forceful grasping or lifting. Tennis elbow begins as microtears of the origin of the extensor carpi radialis brevis (ECRB), and may also involve the extensor carpi radialis longus (ECRL) and extensor carpi ulnaris (ECU). In patients with lateral epicondylitis, there is a delay or failure of healing of these tissues. Golfer’s elbow involves the origin of the common flexor tendon, and has a similar process of healing
Both Tennis or Golfer's elbow typically lasts for 6-24 months, with between 70-90% resolving by one year. For the vast majority of people, they will resolve on their own and leave you with a normal elbow. Understanding these conditions and utilizing conservative measures helps ease the pain during the healing process, helps patients and doctors navigate a prolonged experience, and helps one take an active role in the healing process.
Are there any non-surgical treatments?
The first line of treatment includes activity modification, braces, heat/ice, stretching, and anti-inflammatory medications.
- Stretching: Many people feel that stretching is more effective after applying heat to the elbow.
- Braces: These are useful for the management of symptoms, primarily to relieve pain. They can be worn at the patient's convenience and are often used in demanding tasks or specific situations.
- Medications: The most common medications are anti-inflammatory medications. These can range from over-the-counter medications such as Advil or Aleve to the prescriptions/medicines often used and called non-steroidal anti-inflammatory drugs. Names that may be familiar include Naprosyn, Ibuprofen, Sulindac, Meloxicam as well as many others. These medicines are generally safe. Their side effects, however, can be significant and need to be monitored. Specifically, to minimize GI side effects like nausea, anti-inflammatory medications should be taken with food. They are excreted from the body through the kidneys, so it is crucial to maintain good hydration. Periodic blood tests should be used to assess kidney function. These blood tests can be coordinated with your regular primary care physician.
- Injections: Only recommended in cases where functional activities of daily living are compromised. To date, the only acceptable injections are cortisone-type, whole blood, and PRP injections.

What if the non-surgical options do not work for me?
Rarely (5-10%), when all conservative measures have failed, symptoms continue to be extreme, and the duration of symptoms is prolonged, surgical treatment is considered. This involves removal of the compromised tendon tissue and repair of the surrounding healthy structures.