
Are you suffering from symptoms of a trigger finger?
The Omaha Hand & Wrist Specialists at MD West ONE are able to properly diagnose and treat trigger fingers through both surgical and non-surgical treatments. If you have the following symptoms, you may want to make an appointment with one of our Board Certified Specialists.
- Finger stiffness, especially in the morning
- A popping or clicking sensation when moving your finger
- Tenderness or lump in the palm of your hand at the base of the finger
- Finger catches or locks at a bent position and then suddenly pops straight
Trigger Finger: Non-surgical and Surgical Treatment(s)
TRIGGER FINGER
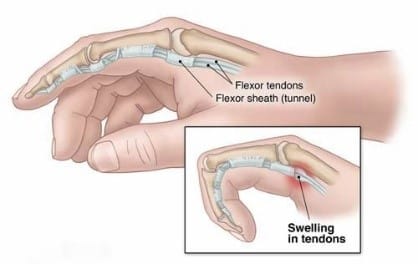
A trigger finger is a very common condition that presents with catching and locking of an individual finger with pain over the base of that finger.
The actual triggering is due to the catching of a small benign nodule on the flexor tendon at the level of the first pulley. (The pulleys are the ligament-like bands that hold the tendon near the bone). It can present at any age, literally from birth to into the 90s. The majority are found in middle-aged patients. It may involve one or more fingers at a time.
Conditions that are associated with soft tissue inflammation have been correlated with the development of trigger fingers. These conditions include diabetes mellitus, thyroid abnormalities, inflammatory arthritis, and other conditions. There is some correlation between heavy repetitive hand use and the development of trigger fingers.
INITIAL CARE IS CONSERVATIVE
For the hand physicians at MD West ONE, the treatment includes the utilization of multiple modalities.
- Medications: We usually use anti-inflammatories. This may vary from over-the-counter medications such as Ibuprofen (Advil), Naprosyn (Aleve), and/or other anti-inflammatories.
- Braces: Research done by the physicians at MD West ONE shows that utilization of an extension splint can be helpful. We encourage the utilization of any of several types of splints as long as they hold the finger in full extension. Currently, we are only using these splints at night as they can be cumbersome during the day.
- Injections: Cortisone-type injections have been shown to be very helpful for the treatment of trigger fingers. Studies evaluating the use of cortisone injections show these can be repeated, and a significant resolution of symptoms occasionally will involve utilization of up to four injections. Timing-wise, these should be spread out over months in general.
- Exercises: There is no exercise regimen for trigger fingers. That said, warm-up stretching exercises for the wrist and fingers would be very reasonable to minimize the risk of inflammation and the development of trigger finger symptoms.
SURGICAL ALTERNATIVES
If the conservative measures fail for a trigger finger, there are a couple of surgical options. These have evolved over the last several years. Surgeons have the preference depending on their experience and training. Currently, we utilize two types of surgical therapies.
In-office ultrasound-guided percutaneous trigger finger release
A percutaneous trigger finger release has been utilized by hand surgeons for many years. With the integration of ultrasound into our offices, we believe this can be done safer and with direct visualization of the surgical equipment. This ultrasound visualization, we believe, helps minimize trauma to the soft tissues during a trigger finger release. This procedure is done in the office under local anesthesia. We usually schedule a little extra time in our office to do these. At the time of this procedure, we will localize adjacent nerves and arteries and the midline of the tendon by ultrasound. With the use of local anesthesia, we will minimize the pain associated with the intervention. Standard surgical prep and draping will be performed. After adequate anesthesia is obtained, an 18 gauge needle is advanced under ultrasound guidance through the skin and down into the area of the A1 pulley. With the sharp edge of the needle, we can release the pulley. This technique is done advancing from distal to proximal and usually involves three and possibly four percutaneous placements of the needle. Aftercare involves just a compressive hand dressing for 24 hours. Thereafter patients can return to their functional use of the hand. There may be some postoperative swelling and soreness, which may persist for one week or so.
Open surgical trigger finger release
This procedure is done as an outpatient under local and/or sedation anesthesia. At the time of the actual surgery, after appropriate anesthesia is obtained, approximately a 1 cm incision is made in the palm over the area of the triggering (A1 pulley). The A1 pulley is released under direct vision. The tendons can be evaluated. The skin closure includes approximately three to four sutures. A bulky hand dressing is applied for one day or two. The sutures are left in for 10 days. Post-procedure, one needs to do appropriate wound and suture care. One can return to light duty-type activities and slowly progress as comfort allows. With postoperative rehabilitation, it is not necessary to wear splints and/or any type of casting. That patient can resume work with restrictions only as necessary for local discomfort. A home exercise stretching program is all that is necessary. Otherwise, the overall use of that hand can be advanced as tolerated.
Meet MD West ONE's hand specialists and learn more about how they treat trigger finger...




AMERICAN SOCIETY FOR SURGERY OF THE HAND
All of the hand surgeons in the practice are recognized members of the American Society for Surgery of the Hand. It is the oldest and most prestigious medical society dedicated to the hand and upper extremity. The mission of the society is to advance science and practice of hand and upper extremity surgery through education, research, and advocacy on behalf of patients and practitioners. These physicians dedicate their time and energy to improving the patient experience and their knowledge in their field. For more information visit https://www.assh.org.
Functional distal interphalangeal joint splinting for trigger finger in laborers: a review and cadaver investigation.
Rodgers JA1, McCarthy JA, Tiedeman JJ.